Methods
Trial design
- Subjects had an ILD other than IPF, diagnosed according to the investigator’s usual clinical practice; diffuse fibrosing interstitial lung disease of >10% extent on HRCT; FVC ≥45% predicted; DLco ≥30%–<80% predicted.
- Subjects met ≥1 of the following criteria for ILD progression in the 24 months before screening, despite management deemed appropriate in clinical practice:
- Relative decline in FVC ≥10% predicted
- Relative decline in FVC ≥5–<10% predicted and worsened respiratory symptoms
- Relative decline in FVC ≥5–<10% predicted and increased extent of fibrosis on HRCT
- Worsened respiratory symptoms and increased extent of fibrosis on HRCT.
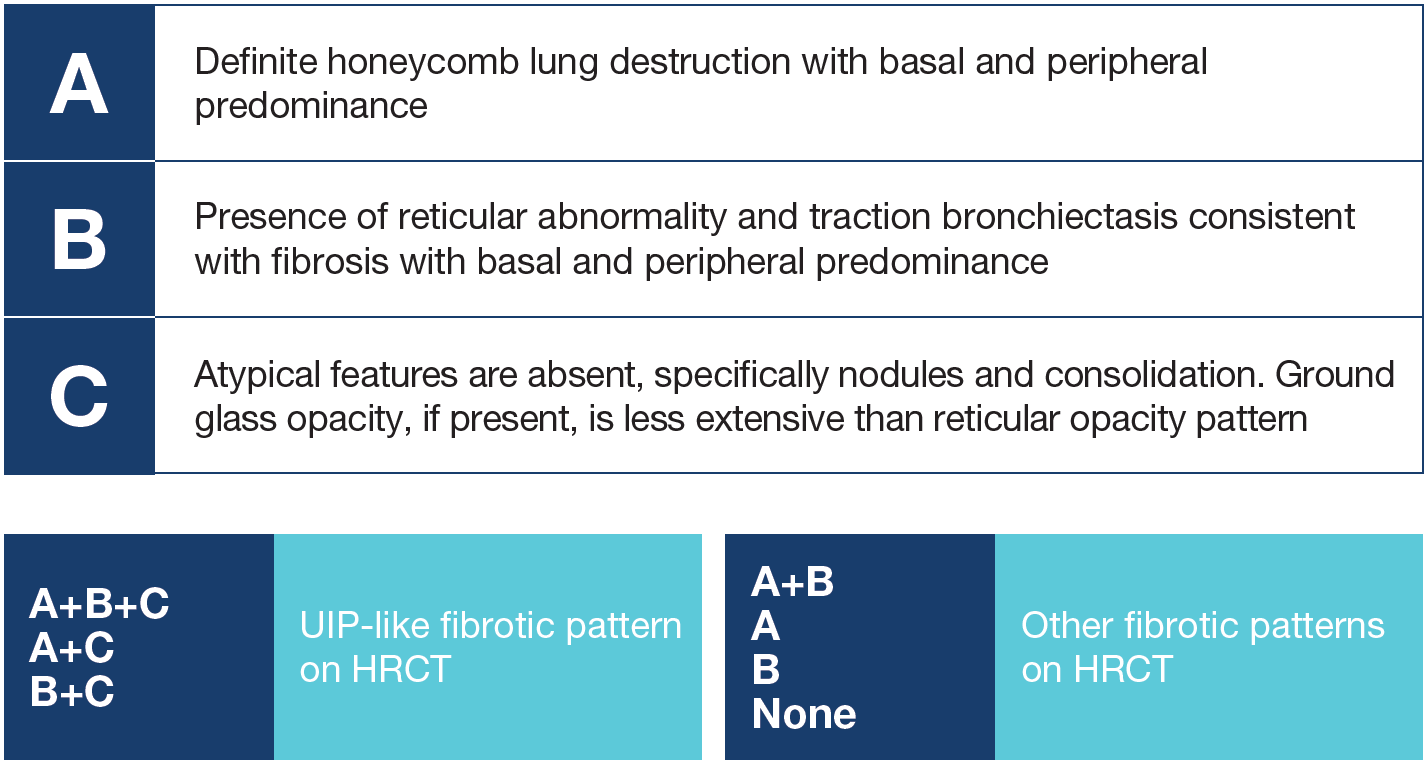
- Subjects were randomized 1:1 to receive nintedanib 150 mg bid or placebo, stratified by HRCT pattern (UIP-like fibrotic pattern or other fibrotic patterns) based on central review by expert radiologists. There were two co-primary analysis populations: the overall population and subjects with a UIP-like fibrotic pattern on HRCT.
Fibrotic patterns on HRCT
Analyses
- In pre-specified analyses, we assessed the effect of nintedanib versus placebo on the following endpoints over 52 weeks in subgroups with a UIP-like fibrotic pattern and other fibrotic patterns on HRCT at baseline:
- Rate of decline in FVC (mL/year)
- Change from baseline in K-BILD questionnaire total score
- Time to acute exacerbation or death
- Time to absolute decline from baseline in FVC ≥10% predicted or death.
- Interaction p-values were calculated to assess potential heterogeneity in the treatment effect of nintedanib versus placebo between subgroups. No adjustment for multiplicity was made.